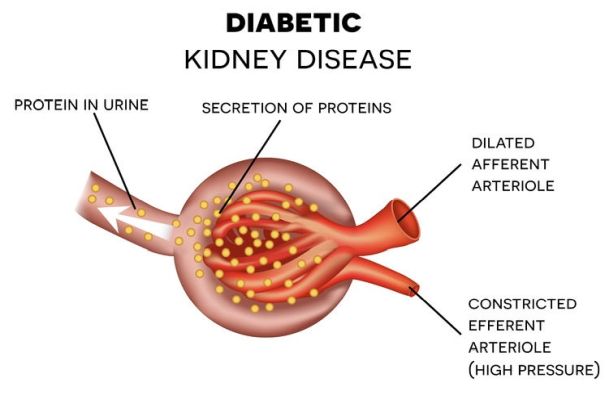
 Diabetes is the leading cause of kidney failure in the developed world, says the best nephrologist in Delhi. The diabetes, characterized disease excess blood glucose can affect various organs of the body including the kidneys (diabetic nephropathy) or eyes (diabetic retinopathy). Good diabetes control is able to prevent, delay or decrease the appearance of these and other complications of the disease. The constant maintenance of high levels of glucose (sugar) in the blood causes a disturbance in the wall of the arteries. As a consequence, the blood does not correctly reach the tissues and this leads to a disorder in the structure and function of different organs in the body, explains the nephrologist in Delhi. The mechanism by which excess glucose affects the arteries is very complex. On the one hand, the wall of the arteries is made up of proteins. Glucose tends to bind to these proteins, and this phenomenon can ultimately deconstruct the arterial wall. On the other hand, the insulin deficiency characteristic of diabetes means that the transformation of glucose for energy is carried out through a specific type of metabolic pathway. As a consequence, the body accumulates a series of substances that can also cause alterations in the walls of the arteries, says the nephrologist in Noida. The appearance of complications in a diabetic person also depends on their personal susceptibility to changes caused by high glucose levels. Diabetes is the leading cause of kidney failure in the developed world, accounting for approximately 35-40% of new cases of kidney failure each year, says the nephrologist in Gurgaon. It should be known that: – The development of early stages of diabetic nephropathy is frequent Throughout life, around 50% of people with type 1 diabetes develop microalbuminuria – presence of the albumin protein in the urine, which is an indicator of impaired kidney function. – Approximately 20% of people with type 1 diabetes develop kidney failure. In Caucasian people with type 2 diabetes, between 5 and 10% go on to develop end-stage chronic kidney failure (CRFD), while among non-Caucasians the proportion is even higher. Diabetic kidney failure is the most common cause of admission to kidney replacement programs, dialysis or transplantation, in most countries of the world, says the kidney transplant doctor in Delhi. In India, around a third of people with end-stage chronic kidney disease have diabetes. This population is estimated to grow at an annual rate of 8%. – Up to 40% of new cases of IRCT can be attributed to diabetes. The risk of CKD is 12 times higher in people with type 1 diabetes compared to those with type 2 diabetes, says the kidney specialist in Delhi. –There are two treatment options when the kidneys fail. Dialysis – peritoneal dialysis or hemodialysis – and kidney transplant. The costs of both treatments are high. Diabetes is estimated to represent between 5 and 10% of the national health budget in western developed countries. – Diabetic kidney failure develops so slowly that it may not give symptoms for many years. The best way to detect the problem is to test your urine for proteins, which should not normally be present, such as albumin. The Kidney Specialist in Noida recommends that every person with diabetes undergo a urine test for albuminuria each year. – Close control of the blood glucose level reduces the risk of microalbuminuria, and therefore of future chronic terminal renal failure, by up to 35%. There is conclusive evidence that good blood glucose levels can significantly reduce the risk of developing complications and slowing their progression in all types of diabetes. Control of high blood pressure and high levels of fats in the blood (hyperlipidemia) is also very important, says the nephrologist in Delhi.
0 Comments
 Most kidney diseases can behave like " silent killers ": they work undisturbed, without symptoms, for years and, when their effects are revealed, it can be late to run for cover. Attention to them is dictated by the need to prevent chronic renal failure and to reduce cardiovascular risk, which increases significantly already in the presence of mild renal failure. We cannot therefore think that our kidneys are indestructible, or worse that they do not deserve any consideration; we don't even have to think that kidney disease is always a deadly trap. If the diagnosis is early, the treatments can be very effective. A healing is common. In any case, the evolution of the disease can be significantly slowed down, says the nephrologist in Delhi. So, what can you do to find out about kidney injuries in time? First of all, be careful of the signs that may indicate their appearance. Here are the main ones:
First of all, a fresh urine test must be performed (to avoid alterations caused by fermentation). Most kidney diseases cause urinary changes, with the presence of:
A separate case is that of cancer cells that can be highlighted by the so-called urinary cytological examination. Abnormal amounts of albumin, blood and white blood cells can be easily searched for by immersing a test strip in the urine. It is this safe and rapid research method that is used in the screening of kidney disease. In case of abnormality, the examination will be supplemented by the microscopic one of the urinary sediments. Very reliable and rapid automatic equipment is now spreading in the most modern laboratories, which allow to combine the chemical examination with that of the urinary sediment. As always happens in medicine, there are exceptions to the kidney disease rule = urinary alterations. The most common exception is that of nephroangiosclerosis and some hereditary diseases, at least in the initial phase, such as polycystic kidneys, which can be present without there being obvious urinary changes. It should also be borne in mind that, in the course of their progression towards an ever more serious renal failure, chronic kidney diseases often cause arterial hypertension. In turn, kidney damage can be caused by an arterial hypertension that is not initially linked to nephropathy (by far the most common condition is that of the so-called essential arterial hypertension). Measuring blood pressure is therefore another important step to discover nephropathy in time and, often, to prevent it. A simple urine test and a blood pressure check therefore allow you to suspect the existence of a kidney disease, but unfortunately the normal results are not enough to rule it out categorically. For this reason, it is necessary to identify people at risk of developing nephropathy in order to subject them to more detailed investigations. Detecting the presence of a condition at risk of developing nephropathy, and not rarely if more than one is associated with it, is however very important if you want to prevent the onset of kidney damage. To prevent kidney disease, the most important risk conditions for their appearance must be taken into account and, if possible, prevented and corrected, suggests the nephrologist in Noida. Here are the main risk conditions for the development of a kidney:
Taking these conditions into account, nephrologist in Delhi suggests some good rules for defending our kidneys. 1. Prevention means first of all treating diseases that can induce kidney damage: first of all arterial hypertension, arteriosclerosis and diabetes. Naturally, first of all, the conditions that can favor their appearance must be corrected, such as obesity, the so - called dysmetabolic syndrome, too sedentary life, varying, if necessary, the lifestyle. 2. In keeping with the previous rule, avoid diets very rich in calories, sugar, sweets, animal fats and salt, and smoking. The traps are many. Canned and preserved foods are generally rich in salt; even the bread of some regions is quite rich: in case of need, consuming bread without salt can be useful. It is always good to drink water with a certain abundance: a liter and a half or two a day is a safe dose. The smoke can also be harmful to the health of the kidneys, warns the nephrologist in Gurgaon. 3. Do not resign yourself to living with high cholesterol and excess body weight, which can promote arteriosclerosis, high blood pressure and diabetes. 4. Regularly check the blood pressure, knowing that it is considered an optimum pressure equal to or less than 130 of 80 mm of mercury, and that values above 140/90 are defined as pathological, at any age (although in diabetics is suggested keep the pressure at values lower than 130/80), suggests the kidney specialist in Delhi. 5. If you are hypertensive, have diabetes or signs of arteriosclerosis, also take care to protect the kidneys, by implementing all the measures recommended by the doctor for kidney in Delhi. However, it is not enough to be content with following treatments: it is also necessary to check that the results are really what you want. For example, in the case of high blood pressure, the treatment can be considered effective only if blood pressure values lower than the classic "140 out of 90" are obtained. Today there are many drugs to control arterial hypertension and it is often obtained by combining several medicaments in small doses, with reduction of negative side effects and enhancement of the positive effect. It is also important to know that some of these drugs, such as ACE inhibitors and so-called receptor antagonists, in addition to the antihypertensive effect, also have a specific renoprotective action. 6. In the case of diabetes, make sure to obtain well-controlled glycemic levels, with values of the so-called glycated hemoglobin as close as possible to the norm, and also in this case check blood pressure very well and resolve any overweight conditions, says the kidney specialist in Noida. 7. Maintaining a proper diet and careful control of body weight, which is always important: taking medications does not authorize you to neglect dietary rules. 8. Do not resign yourself to living with urinary tract infections, kidney stones or chronic obstruction of the urinary tract, for example from prostatic hypertrophy. 9. Avoid prolonged use of potentially nephrotoxic drugs, such as analgesics or anti-inflammatory drugs, especially if taken without medical supervision; this does not mean that those who need it should give it up, but it is advisable, if you use them frequently, to remember to check the kidney situation periodically, advices the kidney specialist in Gurgaon. 10. Carry out, even if it feels good, a simple urinalysis during other laboratory tests, or in any case with a two-year deadline, and do not neglect any minor anomalies revealed by the urinalysis, such as blood or proteins in very large quantities modest. On the other hand, it should not be forgotten that in some situations, such as in the presence of kidney damage due to high blood pressure or arteriosclerosis, the urine test is often normal for a long time. 11. Perform, under all risk conditions, a check on renal function with the determination of creatininemia, possibly repeating it at regular intervals, for example annual, or every six months if the risk is high. Creatinine is a muscle mass product which is eliminated by the kidney and accumulates in the blood when kidney function decreases. Blood values above 1.2 mg / dl in women and 1.4 mg / dl in men may indicate functional kidney damage and warrant further investigation. Using simple mathematical formulas and commonly used calculators it is easy to deduce the value of renal filtration from creatininemia. This control, which has supplanted the traditional one of blood urea nitrogen, can constitute a first alarm bell, particularly important when the urine test is normal, for an evolutionary nephropathy. 12. Be careful of minor and nonspecific signs of kidney disease, such as edema of the lower limbs, hypertension, even if not constant, chronic or relapsing urinary tract infections, the emission of urine of a different color or odor than usual. All these signs do not always indicate the presence of kidney disease or urinary tract, but it is best to make sure that they are truly harmless, suggests the nephrologist in Delhi.  The therapeutic objectives of referral to a nephrologist in Delhi are aimed at reducing and treating the associated complications of CKD, and preparing adequately and sufficiently in advance, the replacement treatment for renal function. Early detection and appropriate referral to Nephrology of patients with CKD reduces complications and improves long-term survival, since it allows early identification of reversible causes, decrease the rate of progression, decrease associated cardiovascular morbidity and mortality, and prepare the patient adequately for dialysis if necessary. The improvement of the care and the prognosis of CKD must be made through early detection plans in the population at risk, which implies close coordination and collaboration between Primary Care and Nephrology, says the nephrologist in Noida. According to the nephrologist in Delhi, the treatment of Chronic Kidney Disease aims to avoid or reduce risk factors for disease progression, prevent the onset of symptoms and minimize complications. The low protein diet delays the appearance of excess urea symptoms (pruritus, insomnia, neurological, neuromuscular, gastrointestinal and other disorders), by reducing its generation. Although controversial, it is suggested that protein restriction slows the progression of CKD. This concept is not applicable to patients with polycystic kidney disease, but protein restriction is especially beneficial in diabetic nephropathy, says the nephrologist in Gurgaon. Before prescribing the diet, the patient must undergo a nutritional evaluation. Also, the diet must include an adequate energy supply. There is a favourable circumstance that phosphorus restriction is proportional to protein restriction, so both guidelines are consistent. In addition, the low protein diet prevents part of metabolic acidosis, by reducing the generation of acids in the body. A low protein diet is especially useful in patients with CKD grade 4 and 5, although it is less important if the patient has very well controlled blood pressure. The low protein diet can cause malnutrition, so it should be provided between 0.6 and 0.8 g / kg / person / day, in those with moderate-severe or severe kidney failure, and some parameters should be evaluated periodically corporal like the index of corporal mass, the triceps fold or the circumference of the arm, and biochemicals (in the analytical ones) like albumin and serum cholesterol, or lymphocyte levels. On the other hand, the diet must contain 35-40 kilocalories per kilogram of weight per day, suggests the kidney specialist in Delhi. With a low protein diet, acid production is reduced, but despite this, in an advanced CKD situation, the kidney is not capable of producing the bicarbonate necessary to replace what is lost, and it is necessary to replace it as a supplement (3 -4 grams daily in the form of oral stamps or bicarbonated water). This amount depends on kidney function and the animal protein content of the diet, explains the kidney specialist in Noida. The water intake depends on the diuresis that is conserved. Diet salt is often limited to control excess fluids and high blood pressure. However, the loss of the ability to dilute urine associated with CRF implies that a minimum intake of salt is necessary to guarantee that the patient can eliminate, for example, 2 liters of water; otherwise water is retained, and sodium in the blood drops too low (hyponatremia). This process is frequent during hospitalization, in which very restrictive diets can be indicated in salt and liquids are provided in the form of glucose serum. Salt restriction reduces the sodium load reaching the end places of the nephron where sodium is exchanged for potassium (the tubule reabsorbs sodium and expels potassium), thus favouring the dangerous increase in potassium in the blood (hyperkalemia), says the kidney specialist in Gurgaon. The different alterations in bone-mineral metabolism (hyperphosphoremia, hypocalcaemia, hyperparathyroidism, osteoporosis, etc.) are secondary to the progressive loss of mass and kidney function. As glomerular filtration decreases, a discrete but significant decrease in calcitriol can be seen secondary to the loss of renal mass, and to phosphate retention, which in turn decreases the renal synthesis of calcitriol. Furthermore, with this deficit of calcitriol synthesis, intestinal calcium absorption decreases, producing hypocalcemia. The positive balance of phosphorus, the deficit of calcitriol and the hypocalcemia, lead to an increase in PTH and trigger a situation of secondary hyperparathyroidism. Control of the phosphocalcium balance is essential to prevent it, and its values must be kept in range according to the degree of renal failure of the patient. The basic treatment is with phosphorus chelating drugs, which manage to “catch” it from the diet and eliminate it with the faeces. A normal diet provides about 1,200 mg of phosphorus a day; When urinary phosphorous excretion is less than 700 mg / day, hyperphosphoremia and stimulation of PTH secretion begin to occur. At this time, emphasis should be placed on restricting foods rich in phosphorus, and if necessary, combining chelators and vitamin D, suggests the doctor for kidney in Delhi. People with Chronic Kidney Disease have a much higher cardiovascular risk than the general population, and it is essential to fight all the factors that increase that risk. It is as important to try to slow down the progression of CKD as to combat factors such as high blood pressure, excess cholesterol, obesity, which multiply the complications in these vulnerable patients. Most patients with CRF have anemia, due to the relative deficit of renal synthesis of erythropoietin. Specific treatment improves survival, decreases morbidity, and increases quality of life in both dialysis and pre-dialysis patients, says the nephrologist in Delhi. Tobacco use is the most common cause of preventable cardiovascular mortality worldwide. The immediate deleterious effects of smoking are related to activation of the sympathetic nervous system, which increases myocardial oxygen consumption through an increase in blood pressure, heart rate, and myocardial contractility. Furthermore, smoking induces a progressive increase in arterial stiffness and is a major risk factor for cardiovascular disease, coronary heart disease and cerebrovascular disease. Furthermore, tobacco induces and accelerates the progression of CKD. In patients with advanced CKD, smoking is a cardiovascular risk factor and is associated with an increased risk of developing heart attacks, peripheral vascular disease, heart failure, and mortality. Quitting smoking is an essential therapeutic goal in CKD patients. |
AuthorA passion for helping others led me down the path of Medicine into a career that allows me to provide my patients with high quality healthcare. As a professional Nephrologist in Delhi since 2008, I bring a holistic approach to medicine in order to find comfortable and effective solutions for everyone. Read on to learn more about my medical background. Archives
March 2023
Categories |

 RSS Feed
RSS Feed
